Rapid Response Team (RRT)

Within the framework of clinical quality improvement and Patient Safety, the Rapid Response Team (RRT)—also known as the Medical Emergency Team (MET)—is a vital clinical strategy designed to prevent the physiological deterioration of hospitalized patients outside the Intensive Care Unit (ICU).
The core premise is that in-hospital cardiopulmonary arrest (CPA) is rarely a sudden, unpredictable event. It is frequently preceded by hours of physiological instability (measurable changes in vital signs) that, if detected and treated early, can prevent "failure to rescue" and reverse deterioration.
Implementation & Objectives
Implementing an RRT aims to achieve critical hospital safety and quality benchmarks:
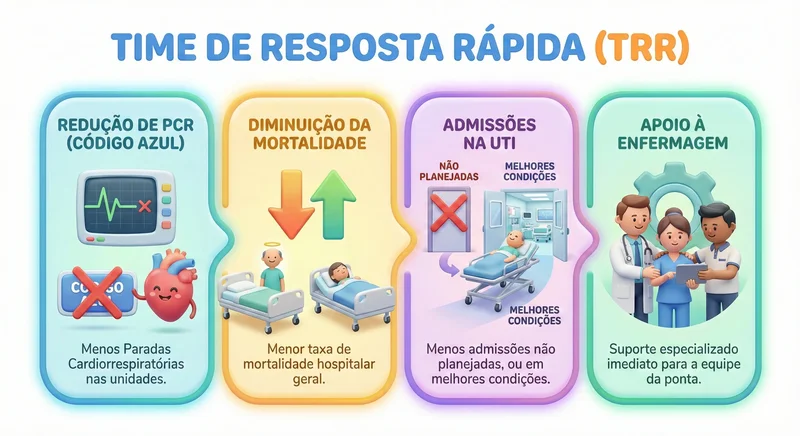
- Reduce the incidence of Cardiopulmonary Arrests (CPA) in medical-surgical wards (Code Blue).
- Decrease overall in-hospital mortality rates.
- Reduce unplanned ICU admissions, or ensure that when transfers are necessary, they occur under controlled, optimized clinical conditions.
- Empower and support bedside nursing staff with immediate, specialized clinical backup.
Structure of a Rapid Response System (RRS)
A comprehensive Rapid Response System is not just a clinical team, but a structured process composed of two primary "limbs" and an administrative component:
Afferent Limb (Detection & Activation)
This is the continuous surveillance system. It involves bedside nursing staff (RNs and clinical technicians) identifying early warning signs of clinical deterioration.
Tools
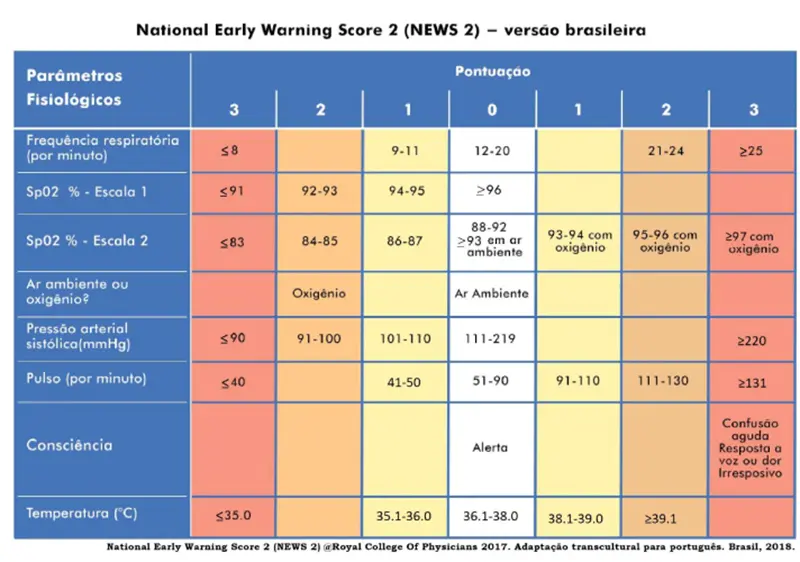
Utilization of standardized early warning scoring systems, such as the National Early Warning Score (NEWS/NEWS2) for adults or the Pediatric Early Warning Score (PEWS) for children.
Action
Upon identifying a clinical "trigger" (elevated score or critical vital sign deviation), the bedside team immediately activates the RRT.

Efferent Limb (Response)
This is the dedicated clinical team that responds directly to the bedside call.
Typical Composition
An ICU-trained physician (intensivist or hospitalist), a Critical Care Registered Nurse (CCR), and a Respiratory Therapist (RT).
Action
Immediate bedside assessment, patient stabilization, and determination of disposition (maintaining ward care with updated orders or transferring to the ICU).
Administrative Component (Governance & Quality Improvement)
Data monitoring and review for continuous quality improvement.
Key Performance Indicators (KPIs): Total RRT activations, response times, CPA rates per 1,000 discharges, and overall hospital mortality.
4. Activation Criteria (Common Triggers)
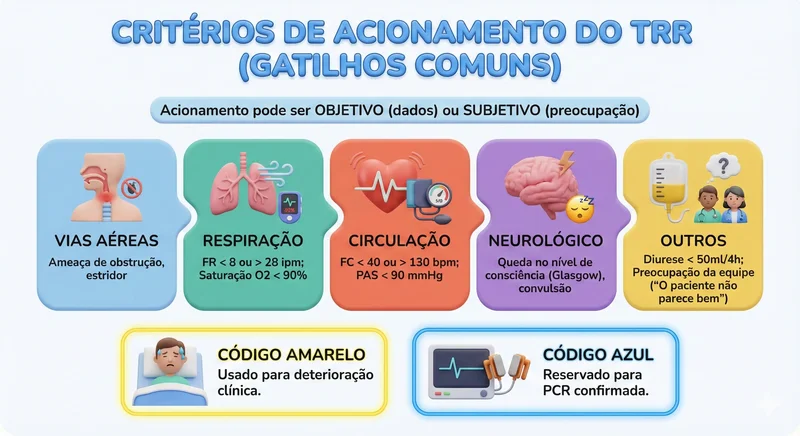
Clinical guidelines emphasize that RRT activation can be objective (data-driven) or subjective (clinician worry/gut feeling).
Warning Vital Signs (Examples)
| Parameter | Activation Criteria (Example) |
|---|---|
| Airway | Threatened airway, stridor, severe respiratory distress |
| Breathing | RR < 8 or > 28 bpm; SpO2 < 90% on oxygen |
| Circulation | HR < 40 or > 130 bpm; SBP < 90 mmHg |
| Neurology | Acute drop in consciousness (GCS), new-onset seizure |
| Other | Urine output < 50mL over 4 hours; Staff concern ("The patient doesn't look right") |
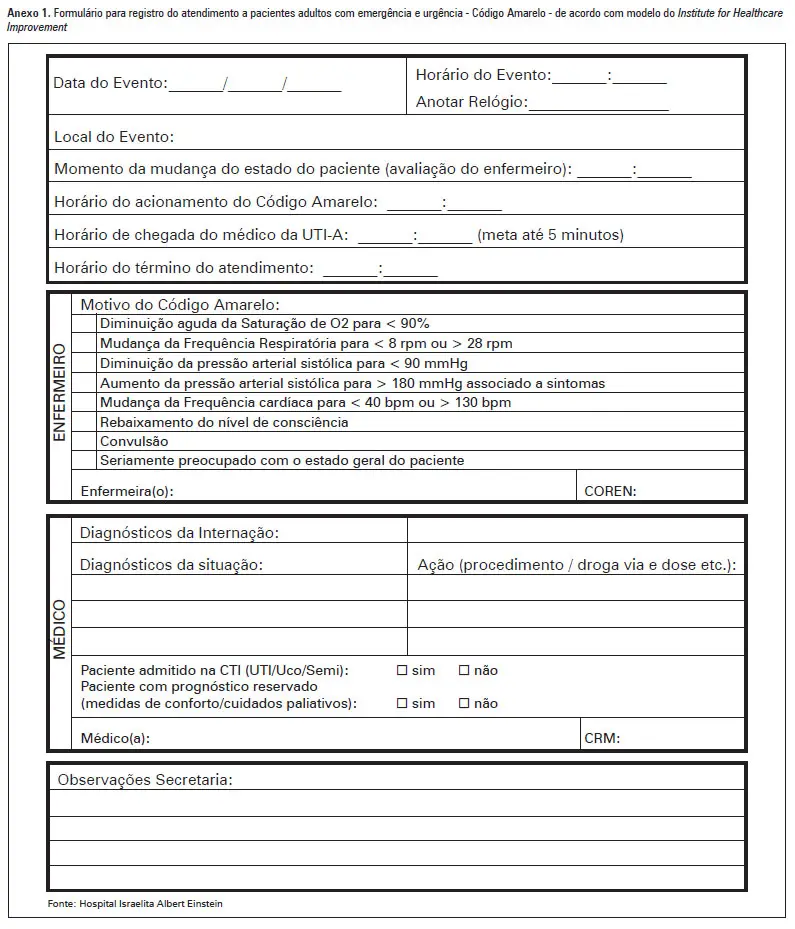
Note: "Code Yellow" (or RRT call) is typically used for acute clinical deterioration, whereas "Code Blue" is strictly reserved for confirmed cardiopulmonary arrest.
Steps for RRT Implementation (Quality Improvement Roadmap)

- Stakeholder Engagement: Securing buy-in from hospital leadership and frontline clinical staff.
- Protocol Standardization: Selecting early warning scores (MEWS/NEWS2) and establishing clear communication pathways.
- Education & Empowerment: Training ward staff to recognize clinical deterioration and empowering them with "no-fault" activation authority.
- Infrastructure & Resources: Securing dedicated equipment (crash carts, defibrillators) and reliable communication channels (dedicated pagers, RRT phones).
- Continuous Quality Improvement (PDCA): Auditing RRT events, analyzing "failure to rescue" cases, and refining processes.
Conclusion
The RRT shifts hospital culture from a reactive "rescue" model to proactive prevention. Within patient safety frameworks, it integrates care, ensures patients receive the right intervention at the right time, and empowers nursing staff through clear communication channels and clinical support.
Here at Nursing Calculators, we offer an automated NEWS (National Early Warning Score) Calculator. Simply input your patient's clinical parameters to instantly determine if they meet the criteria for RRT activation!
Institute for Healthcare Improvement (IHI). Establish a Rapid Response System. Available at: ihi.org
National Institute for Health and Care Excellence (NICE). Acutely ill adults in hospital: recognising and responding to deterioration (Clinical Guideline CG50). Available at: https://www.nice.org.uk/guidance/cg50
The Joint Commission. National Patient Safety Goals (NPSG) - Goal 15: Identify patient safety risks (Rescue protocols). Available at: https://www.jointcommission.org